Blood-brain barrier and immune checkpoint inhibitors
My partner has a recurrent and unoperable glioblastoma.
He is considering a therapy with immune checkpoint inhibitors (e.g. pembrolizumab or atezolizumab) as his tumor has extremely high mutation burden. Some doctors are in favour but some are not convinced and say that it won't work because of blood brain barrier (BBB).
Is there any research showing immune checkpoint inhibitors don't cross BBB?
Tuesday, 30 January 2018
Chloroquine for GBM with EGFRvIII mutation
EGFRvIII expression triggers a metabolic dependency and therapeutic vulnerability sensitive to autophagy inhibition
http://www.tandfonline.com/doi/pdf/10.1080/15548627.2017.1409926?needAccess=true
Some of the data contained in this study was used as justification for the CHLOROBRAIN trial
https://clinicaltrials.gov/ct2/show/NCT02378532
http://www.tandfonline.com/doi/pdf/10.1080/15548627.2017.1409926?needAccess=true
Some of the data contained in this study was used as justification for the CHLOROBRAIN trial
https://clinicaltrials.gov/ct2/show/NCT02378532
Final results of disulfiram pilot trial for newly diagnosed GBM
Final results of a phase I dose-escalation, dose-expansion study of adding disulfiram with or without copper to adjuvant temozolomide for newly diagnosed glioblastoma
http://sci-hub.la/https://link.springer.com/article/10.1007/s11060-018-2775-y
Sadly, median PFS and OS were not improved above historical controls receiving standard treatments alone.
However, only 6 of 18 patients also took copper supplements in this trial in addition to disulfiram, leading to another phase 1/2 trial of disulfiram + copper for newly diagnosed GBM which is still recruiting.
https://clinicaltrials.gov/ct2/show/NCT02715609
http://sci-hub.la/https://link.springer.com/article/10.1007/s11060-018-2775-y
Sadly, median PFS and OS were not improved above historical controls receiving standard treatments alone.
However, only 6 of 18 patients also took copper supplements in this trial in addition to disulfiram, leading to another phase 1/2 trial of disulfiram + copper for newly diagnosed GBM which is still recruiting.
https://clinicaltrials.gov/ct2/show/NCT02715609
Intravenous zoledronic acid for cocktail?
There are many articles on the possible benefits zoledronic acid in the treatment of glioblastoma.
https://www.ncbi.nlm.nih.gov/pubmed/?term=Zoledronic+glioblastoma
For example, MTZ Regimen (2016) suggests using:
oral minocycline 100 mg three times daily, oral telmisartan 80 mg twice daily, and intravenous zoledronic acid 4 mg once every 28 days
https://www.dovepress.com/toward-a-noncytotoxic-glioblastoma-therapy-blocking-mcp-1-with-the-mtz-peer-reviewed-fulltext-article-OTT
https://www.ncbi.nlm.nih.gov/pubmed/27175087
Since many patients with glioblastoma include in their cocktails minocycline and telmisartan (or captopril), may be necessary to think about adding an injection of zoledronic acid as non-toxic supplement, 4mg once every 28 days?
https://www.ncbi.nlm.nih.gov/pubmed/?term=Zoledronic+glioblastoma
For example, MTZ Regimen (2016) suggests using:
oral minocycline 100 mg three times daily, oral telmisartan 80 mg twice daily, and intravenous zoledronic acid 4 mg once every 28 days
https://www.dovepress.com/toward-a-noncytotoxic-glioblastoma-therapy-blocking-mcp-1-with-the-mtz-peer-reviewed-fulltext-article-OTT
https://www.ncbi.nlm.nih.gov/pubmed/27175087
Since many patients with glioblastoma include in their cocktails minocycline and telmisartan (or captopril), may be necessary to think about adding an injection of zoledronic acid as non-toxic supplement, 4mg once every 28 days?
Saturday, 27 January 2018
Intraarterial bevacizumab
I found information about the intra-arterial administration of bevacizumab. It looks very interesting.
Does anyone know any details?
Long-term benefit of intra-arterial bevacizumab for recurrent glioblastoma.
2017 https://www.ncbi.nlm.nih.gov/pubmed/28472567
"Standard treatment for recurrent GBM is not yet established. We present a case demonstrating the benefit of intra-arterial (IA) bevacizumab with blood brain barrier disruption (BBBD) for the treatment of recurrent GBM. A 31 year-old man diagnosed with GBM, following primary resection, received temozolomide. After a second resection, he received one dose of IA bevacizumab with BBBD using mannitol, preventing regrowth for 2.5 years. Following tumor regrowth, the patient received another dose of IA bevacizumab with BBBD, which has prevented regrowth for another year."
2012 https://www.ncbi.nlm.nih.gov/pubmed/22946342
Intra-arterial bevacizumab with blood brain barrier disruption in a glioblastoma xenograft model.
Mannitol was used to prepare the solution:
https://www.drugs.com/monograph/mannitol.html
The practice of such treatment in Ukraine:
2013 https://cyberleninka.ru/article/n/ispolzovanie-metoda-vnutriarterialnogo-vvedeniya-himiopreparatov-v-sostave-kompleksnogo-lecheniya-patsientov-s-gliomami-golovnogo
For the intra-arterial administration of drugs, the endovascular technique was used.
"It was found that the method of intra-arterial delivery of chemotherapy is effective and efficient in treatment of patients with malignant gliomas of the brain, can reduce the toxic effects of chemotherapy on the patient, to improve the quality of life for patients."
Does anyone know any details?
Long-term benefit of intra-arterial bevacizumab for recurrent glioblastoma.
2017 https://www.ncbi.nlm.nih.gov/pubmed/28472567
"Standard treatment for recurrent GBM is not yet established. We present a case demonstrating the benefit of intra-arterial (IA) bevacizumab with blood brain barrier disruption (BBBD) for the treatment of recurrent GBM. A 31 year-old man diagnosed with GBM, following primary resection, received temozolomide. After a second resection, he received one dose of IA bevacizumab with BBBD using mannitol, preventing regrowth for 2.5 years. Following tumor regrowth, the patient received another dose of IA bevacizumab with BBBD, which has prevented regrowth for another year."
2012 https://www.ncbi.nlm.nih.gov/pubmed/22946342
Intra-arterial bevacizumab with blood brain barrier disruption in a glioblastoma xenograft model.
Mannitol was used to prepare the solution:
https://www.drugs.com/monograph/mannitol.html
The practice of such treatment in Ukraine:
2013 https://cyberleninka.ru/article/n/ispolzovanie-metoda-vnutriarterialnogo-vvedeniya-himiopreparatov-v-sostave-kompleksnogo-lecheniya-patsientov-s-gliomami-golovnogo
For the intra-arterial administration of drugs, the endovascular technique was used.
"It was found that the method of intra-arterial delivery of chemotherapy is effective and efficient in treatment of patients with malignant gliomas of the brain, can reduce the toxic effects of chemotherapy on the patient, to improve the quality of life for patients."
Carmofur (ASAH1 inhibitor) is more potent than TMZ in killing glioblastoma cells?
I found an interesting study published in November 2017:
https://www.ncbi.nlm.nih.gov/pubmed/29348854
http://www.oncotarget.com/index.php?journal=oncotarget&page=article&op=view&path[]=22637&path[]=71521
"The standard glioblastoma chemotherapy agent, temozolomide, had minimal GSC-targeted effects at comparable or even higher concentrations (IC50 > 750 μM against GSCs). ASAH1 is identified as a de novo glioblastoma drug target, and ASAH1 inhibitors, such as carmofur, are shown to be highly effective and to specifically target glioblastoma GSCs. Carmofur is an ASAH1 inhibitor that crosses the blood-brain barrier, a major bottleneck in glioblastoma treatment. It has been approved in Japan since 1981 for colorectal cancer therapy. Therefore, it is poised for repurposing and translation to glioblastoma clinical trials."
"ASAH1 inhibitors are highly more potent than temozolomide in killing GSCs and U87MG cells. Due to its high level of expression in GSCs, ASAH1 inhibition is proposed as a new anti-glioblastoma therapy that specifically targets GSCs."
2017 https://www.ncbi.nlm.nih.gov/pubmed/28765947
"inhibition of ASAH1 and Sph-1P, either with humanized monoclonal antibodies, small molecule drugs (i.e. carmofur), or a combination of both, led to suppression of GBM cell growth. These results suggest that ASAH1 and Sph-1P may be excellent targets for the treatment of new GBMs and recurrent GBMs, especially since the latter overexpresses ASAH1."

https://www.drugs.com/international/carmofur.html
Unfortunately, I did not find any trials with carmofur (or mifurol) at https://clinicaltrials.gov
https://en.wikipedia.org/wiki/Carmofur
"Carmofur has also been used as adjuvant chemotherapy for curatively resected colorectal cancer patients in China, Japan, and Finland for many years. Trials and meta-analyses have confirmed that the drug is effective on patients with this cancer type, extending their survival.
A clinical trial for small hepatocellular carcinoma was stopped prematurely because 56% of the treated patients had unacceptable side effects. Moreover, the treatment had no survival advantage for stage 1 and 2 cancer patients. This may be a reason why carmofur was never pursued for FDA-approval in the US."
Maybe there are more modern and safe ASAH1 inhibitors crossing the blood-brain barrier?
https://www.ncbi.nlm.nih.gov/pubmed/29348854
http://www.oncotarget.com/index.php?journal=oncotarget&page=article&op=view&path[]=22637&path[]=71521
"The standard glioblastoma chemotherapy agent, temozolomide, had minimal GSC-targeted effects at comparable or even higher concentrations (IC50 > 750 μM against GSCs). ASAH1 is identified as a de novo glioblastoma drug target, and ASAH1 inhibitors, such as carmofur, are shown to be highly effective and to specifically target glioblastoma GSCs. Carmofur is an ASAH1 inhibitor that crosses the blood-brain barrier, a major bottleneck in glioblastoma treatment. It has been approved in Japan since 1981 for colorectal cancer therapy. Therefore, it is poised for repurposing and translation to glioblastoma clinical trials."
"ASAH1 inhibitors are highly more potent than temozolomide in killing GSCs and U87MG cells. Due to its high level of expression in GSCs, ASAH1 inhibition is proposed as a new anti-glioblastoma therapy that specifically targets GSCs."
2017 https://www.ncbi.nlm.nih.gov/pubmed/28765947
"inhibition of ASAH1 and Sph-1P, either with humanized monoclonal antibodies, small molecule drugs (i.e. carmofur), or a combination of both, led to suppression of GBM cell growth. These results suggest that ASAH1 and Sph-1P may be excellent targets for the treatment of new GBMs and recurrent GBMs, especially since the latter overexpresses ASAH1."

https://www.drugs.com/international/carmofur.html
Unfortunately, I did not find any trials with carmofur (or mifurol) at https://clinicaltrials.gov
https://en.wikipedia.org/wiki/Carmofur
"Carmofur has also been used as adjuvant chemotherapy for curatively resected colorectal cancer patients in China, Japan, and Finland for many years. Trials and meta-analyses have confirmed that the drug is effective on patients with this cancer type, extending their survival.
A clinical trial for small hepatocellular carcinoma was stopped prematurely because 56% of the treated patients had unacceptable side effects. Moreover, the treatment had no survival advantage for stage 1 and 2 cancer patients. This may be a reason why carmofur was never pursued for FDA-approval in the US."
Maybe there are more modern and safe ASAH1 inhibitors crossing the blood-brain barrier?
Thursday, 25 January 2018
Need suggestions to incorporate supplements in my mom's cocktail(GBM Patient)
Hi folks,
My mother(Age 47) was diagnosed with glioblastoma(IDH1/2 -ve, Methylated) in September 2017, and it has left me devastated ever since. She has completed her 6 weeks of radiation/chemo and her first cycle of 5/23 temozolomide. Her next cycle of temozolomide starts 5 days from now. I stumbled upon this blog just a week back, and have found this to be immensely helpful and resourceful.
I need help from you guys on what else should I incorporate in my mom's cocktail. Following are the supplements that are present in her cocktail per day already:
Metformin: 500 mg
Boswellia Serratta: 4000 mg
Resveratrol: 400 mg
Fish Oil: 3600 mg DHA+EPA + 400 mg of other omega 3 fatty acids
Curcumin with piperine: 5000 mg
Longvida: 400 mg
Quercetin: 5000 mg
Melatonin: 20 mg
Selinium: 200 mcg
Vitamin ADK supplement with 5000 IU Vitamin D3
Ashwagandha: 500 mg
Garlic: 6 cloves
Ginger: 6 cloves
Dendritic cell therapy: On the cards
Cannabis oil: Dropped because it was suppressing her WBCs
She is also on ketogenic diet and has done about 2 weeks of hyperbaric oxygen. We are looking at two more weeks of hyperbaric oxygen.
I'm looking for more supplements that are good adjuvants to temozolomide/standalone good adjuvants that I should definitely include in my mom's cocktail. It'd be great if you guys could help out in more supplements that I should include, I'm finding it very hard to self medicate my mom. Basis Ben Williams' book and reading several blogs, the following supplements have repeatedly been catching my attention:
1. DCA
2. Chloroquine
3. Care oncology clinic protocol(Metformin + Doxycline + Mobendezole + Atorvastatin)
4. Ruta 6 + Calceria Phos(Not sure if it is a good idea to use while on chemo)
5. Methadone
6. Veramapil
7. Low Dose Naltrexone
8. Disulfiram
9. Perilyl Alcohol
10. Methadone
11. Celebrex
She is already taking a total of 50 meds per day and I think she can take only 10-15 more. Would be great if you can help me from above list/any other supplement that should definitely be a part of her cocktail.
Thank you in advance!
My mother(Age 47) was diagnosed with glioblastoma(IDH1/2 -ve, Methylated) in September 2017, and it has left me devastated ever since. She has completed her 6 weeks of radiation/chemo and her first cycle of 5/23 temozolomide. Her next cycle of temozolomide starts 5 days from now. I stumbled upon this blog just a week back, and have found this to be immensely helpful and resourceful.
I need help from you guys on what else should I incorporate in my mom's cocktail. Following are the supplements that are present in her cocktail per day already:
Metformin: 500 mg
Boswellia Serratta: 4000 mg
Resveratrol: 400 mg
Fish Oil: 3600 mg DHA+EPA + 400 mg of other omega 3 fatty acids
Curcumin with piperine: 5000 mg
Longvida: 400 mg
Quercetin: 5000 mg
Melatonin: 20 mg
Selinium: 200 mcg
Vitamin ADK supplement with 5000 IU Vitamin D3
Ashwagandha: 500 mg
Garlic: 6 cloves
Ginger: 6 cloves
Dendritic cell therapy: On the cards
Cannabis oil: Dropped because it was suppressing her WBCs
She is also on ketogenic diet and has done about 2 weeks of hyperbaric oxygen. We are looking at two more weeks of hyperbaric oxygen.
I'm looking for more supplements that are good adjuvants to temozolomide/standalone good adjuvants that I should definitely include in my mom's cocktail. It'd be great if you guys could help out in more supplements that I should include, I'm finding it very hard to self medicate my mom. Basis Ben Williams' book and reading several blogs, the following supplements have repeatedly been catching my attention:
1. DCA
2. Chloroquine
3. Care oncology clinic protocol(Metformin + Doxycline + Mobendezole + Atorvastatin)
4. Ruta 6 + Calceria Phos(Not sure if it is a good idea to use while on chemo)
5. Methadone
6. Veramapil
7. Low Dose Naltrexone
8. Disulfiram
9. Perilyl Alcohol
10. Methadone
11. Celebrex
She is already taking a total of 50 meds per day and I think she can take only 10-15 more. Would be great if you can help me from above list/any other supplement that should definitely be a part of her cocktail.
Thank you in advance!
Wednesday, 24 January 2018
The importance of re-testing IDH status in IDH "wild-type" low grade gliomas
PATH-36. REPEATING TESTING IN IDH WILD TYPE LGG CASES. THE IMPORTANCE OF NEXT GENERATION SEQUENCING
Link to abstract
"the observation of a particularly favorable outcome in a group of 42 patients with IDH wild type LGG (OS=93.7 months) led us to assess IDH mutation with a more sensitive technique. Next Generation Sequencing (NGS) was used to evaluate IDH status in these tumor samples, and the results of NGS assay were compared with previous findings"
"Twenty-one (50%) of the 42 initial IDH wild type LGGs were found to present IDH mutation when tested with NGS. Four patients had R132H mutation and 17 cases showed other IDH mutations (4 patients with IDH2 mutation, 5 patients with IDH1 R132C mutation, 5 patients with IDH1 R132G mutation and 3 patients with IDH1 R132S mutation)."
"Repeating testing in IDH wild type LGG cases is crucial, as well as the technique used to assess this mutation. NGS is able to find IDH mutations in 50% of patients previously misdiagnosed"
Link to abstract
"the observation of a particularly favorable outcome in a group of 42 patients with IDH wild type LGG (OS=93.7 months) led us to assess IDH mutation with a more sensitive technique. Next Generation Sequencing (NGS) was used to evaluate IDH status in these tumor samples, and the results of NGS assay were compared with previous findings"
"Twenty-one (50%) of the 42 initial IDH wild type LGGs were found to present IDH mutation when tested with NGS. Four patients had R132H mutation and 17 cases showed other IDH mutations (4 patients with IDH2 mutation, 5 patients with IDH1 R132C mutation, 5 patients with IDH1 R132G mutation and 3 patients with IDH1 R132S mutation)."
"Repeating testing in IDH wild type LGG cases is crucial, as well as the technique used to assess this mutation. NGS is able to find IDH mutations in 50% of patients previously misdiagnosed"
Increased expression of androgen receptor (AR) in GBM. Enzalutamide (androgen receptor inhibitor)
SNO 2016 abstract: CSIG-13 ANDROGEN RECEPTOR IS INVOLVED IN GLIOBLASTOMA AND PRESENTS A POTENTIAL THERAPEUTIC TARGET
SNO 2017 abstract: CSIG-24. ANDROGEN RECEPTOR IS A POTENTIAL THERAPEUTIC TARGET IN GLIOBLASTOMA
"Enzalutamide given orally (20 mg/kg three time per week) to nude mice bearing human gliomas (U78MG) resulted in reduction of 72% in tumor volume (p=0.0027) as compared to mice treated with vehicle. We hope that the results of this study together with continued laboratory efforts will lead to a new approach for the treatment of human glioblastoma."
Enzalutamide is an androgen receptor inhibitor approved by the FDA in 2012 for treatment of prostate cancer.
SNO 2017 abstract: CSIG-24. ANDROGEN RECEPTOR IS A POTENTIAL THERAPEUTIC TARGET IN GLIOBLASTOMA
"Enzalutamide given orally (20 mg/kg three time per week) to nude mice bearing human gliomas (U78MG) resulted in reduction of 72% in tumor volume (p=0.0027) as compared to mice treated with vehicle. We hope that the results of this study together with continued laboratory efforts will lead to a new approach for the treatment of human glioblastoma."
Enzalutamide is an androgen receptor inhibitor approved by the FDA in 2012 for treatment of prostate cancer.
PARP inhibitors for PTEN-mutant cancer cells
Most GBM tumors (IDH1 wild-type) have a loss of one copy of chromosome 10. Additionally, about 30% will also have a deactivating mutation in the remaining copy of PTEN, leaving no functional PTEN in these tumors.
In these tumors, PARP inhibitors may be an effective therapeutic option, based on a study showing therapeutic effects of olaparib in PTEN-negative HCT116 colon cancer xenografts, while HCT116 xenografts with restored PTEN didn't respond to olaparib.
These results are not necessarily generally applicable, as the HCT116 line is also known to have mismatch repair defect (loss of MLH1), so there may have been some interaction between loss of both mismatch repair and PTEN that sensitized cells to olaparib.
Study title:
Synthetic lethal targeting of PTEN mutant cells with PARP inhibitors
Full study available here
In these tumors, PARP inhibitors may be an effective therapeutic option, based on a study showing therapeutic effects of olaparib in PTEN-negative HCT116 colon cancer xenografts, while HCT116 xenografts with restored PTEN didn't respond to olaparib.
These results are not necessarily generally applicable, as the HCT116 line is also known to have mismatch repair defect (loss of MLH1), so there may have been some interaction between loss of both mismatch repair and PTEN that sensitized cells to olaparib.
Study title:
Synthetic lethal targeting of PTEN mutant cells with PARP inhibitors
Full study available here
Chloroquine has therapeutic effect in IDH-mutant U87 mouse model

According to this study, 2-hydroxyglutarate produced by the mutant IDH1 enzyme leads to endoplasmic reticulum (ER) stress, autophagy of the endoplasmic reticulum, and reduced biosynthesis of membrane phospholipids (as the ER is the site of phospholipid synthesis). Inhibiting autophagy with chloroquine triggered apoptosis (programmed cell death).
Chloroquine-treated IDH1-mutant U87 tumors had increased caspase activity (a marker of apoptosis), while the IDH1 wild-type U87 tumors had no increase in caspase activity with chloroquine treatment.
Study title:
2-hydroxyglutarate-mediated autophagy of the endoplasmic reticulum leads to an unusual downregulation of phospholipid biosynthesis in mutant IDH1 gliomas
Pubmed link
I've uploaded the full study to the Library (Folder 2 Therapies - preclinical -> Chloroquine)
Best place for dendritic cell therapy for my mom(GBM Patient)
Hi folks,
My mother is a grade 4 brain cancer patient, who was diagnosed on 17 September 2017. She has completed her 6 weeks of radio/chemotherapy and her 1st 5/23 cycle of temozolomide. I'm looking for immunotherapy(dendritic cell therapy), and where to get it done from is something that I'm terribly confused about. I shortlisted the following:
1. IOZK(They say they will do hyperthermia) while my mom is on chemo, and will do the DC after my mom is done with the Chemo. They say they won't be able to use the tumor block because it is stored in paraffin. They tell me they have their own set of GBM antigens that they shall use.
2. Dr Nesselhut: They say they will give 4-6 vaccines of dendritic cells and can be given while on chemotherapy(1 week before or after). But they say that they can use the tumor block for making the antigens, despite the fact that the block is in paraffin. They say they can 'de-parafinise' it. I'm not sure if they really are true with their claims, but they were the only place that said they can use the block to make the antigens
3. Verita Life, Bangkok: They say that they can give the dendritic cell therapy while on chemotherapy with their own set of antigens, but can't use the tumor block. They shall couple the treatment with a lot of herbal IVs like quercetin, curcumin, resveratrol, Vitamin C etc.
4. Dr Robert Godner: They've asked me to wait for another MRI since the recent one came out clean, but with choline elevation(which is either a sign of radiation injury or residual tumor/recurrence).
I wish to know what shall be the best place to get the immunotherapy done from? Would love objective inputs from you guys. I would also want to know how many times you were made to travel to these places, if you've experienced the dendritic cell therapy from them.
PS: My personal preferential order is the order in which I've placed the above places, but IOZK and Dr Nesselhut, I foresee will easily call us to Germany about 8-10 times, which I'm not very sure my mom will be able to go. So, travel for a GBM patient a few months from now is a concern.
Sunday, 21 January 2018
Improvement of the ketogenic diet
In many studies, it has been shown that a ketogenic diet can be a useful supplement in the treatment of glioblastoma. I would like to discuss the improvement of this diet on the basis of recent research.
1. Ketogenic diet + α-lipoic acid and hydroxycitrate
2017 https://www.ncbi.nlm.nih.gov/pubmed/28122260
"To decrease anabolism, glucose uptake should be reduced (ketogenic diet). To increase catabolism, the oxidative phosphorylation should be restored. Treatment with a combination of α-lipoic acid and hydroxycitrate has been shown to be effective in multiple animal models."
2016 http://crescopublications.org/pdf/CROOA/CROOA-2-019.pdf
"Combination of Metabolic Treatment of Aggressive Primary Brain Tumour
and Multiple Metastases of the Brain"
"We report the cases of 12 patients with advanced brain tumor. They were all treated with
conventional treatment and a combination of sodium R lipoate (800 mgbid), hydroxycitrate at 500 mg tid and low-dose naltrexone at 5 mg at bedtime. Eight patients had primary brain tumour (n=8 including five glioblastomas) four patients had multiple brain metastases."
2. Ketogenic diet + Fenofibrate ?
2016 https://www.ncbi.nlm.nih.gov/pubmed/26869992
"Our results reveal a new, intriguing aspect of cancer cell biology and highlight the benefits of fenofibrate as a supplement to both canonical and dietary (ketogenic) therapeutic approaches against glioblastoma."
2015 https://www.ncbi.nlm.nih.gov/pubmed/26172294
"Given that fenofibrate is a widely used non-toxic drug, we suggest its use in patients with glioblastoma multiforme (GBM)."
2017 https://www.ncbi.nlm.nih.gov/pubmed/28459367
"...the lipid-lowering agent fenofibrate...have potential to lower synthesis or effects of G(M)-CSF and thus deprive a glioblastoma of some of the growth promoting contributions of bone marrow and G(M)-CSF.
It's strange, but in this blog I did not find any information about Fenofibrate. So is it necessary to add it to the ketogenic diet?
3. Ketogenic diet
"Inhibition of glutamine metabolism slows the in vitro and in vivo growth of GLNHigh GBM cultures despite metabolic adaptation to nutrient availability, in particular by increasing pyruvate shuttling into mitochondria."
"...the pleiotropic metabolic inhibitor EGCG, targeting glutamine metabolism, specifically reduces tumor proliferation, in vitro and in vivo, of mesenchymal GLNHigh cells."
How can the findings of this study be used? Only EGCG can not inhibit glutamine metabolism. Maybe there are more options?
4. Ketogenic diet
Friday, 19 January 2018
Total resection followed by multimodal immunotherapy: 15+ months remission without RT/TMZ
HGG-05 Can Multimodal Immunotherapy Replace Radiochemotherapy in Completely Resected Adult GBM?
4th Biennial Conference on Pediatric Neuro-Oncology Basic and Translational Research, June 15-16, 2017, New York City
Link to complete abstracts
Link to abstract HGG-05
While this is only a single case, the long duration of remission in the absence of radiation and chemotherapy is intriguing. This patient was also IDH wild-type, and was in EORTC recursive partitioning analysis (RPA) class IV, as are the majority of GBM patients in phase 3 trials.
The patient was treated at IOZK in Germany with "multimodal immunotherapy consisting of 2 cycles of 6 days Newcastle Disease Virus (NDV) infusions and local modulated electrohyperthermia (mEHT) sessions plus an autologous DC vaccine loaded with serum-derived NDV/mEHT-induced antigenic microparticles + NDV, and additionally four more treatments with NDV infusions + mEHT"
More detailed information on IOZK's methods can be found in this publication.
http://www.iozk.de/aktuelles/iozk_austin_oncology_case_reports_2017.pdf
In addition, a technique has been developed at IOZK to use blood serum-derived antigenic microparticles, where no fresh or frozen tumor tissue to produce a tumor lysate is available. This latter method was used in the case report above.
4th Biennial Conference on Pediatric Neuro-Oncology Basic and Translational Research, June 15-16, 2017, New York City
Link to complete abstracts
Link to abstract HGG-05
While this is only a single case, the long duration of remission in the absence of radiation and chemotherapy is intriguing. This patient was also IDH wild-type, and was in EORTC recursive partitioning analysis (RPA) class IV, as are the majority of GBM patients in phase 3 trials.
The patient was treated at IOZK in Germany with "multimodal immunotherapy consisting of 2 cycles of 6 days Newcastle Disease Virus (NDV) infusions and local modulated electrohyperthermia (mEHT) sessions plus an autologous DC vaccine loaded with serum-derived NDV/mEHT-induced antigenic microparticles + NDV, and additionally four more treatments with NDV infusions + mEHT"
More detailed information on IOZK's methods can be found in this publication.
http://www.iozk.de/aktuelles/iozk_austin_oncology_case_reports_2017.pdf
In addition, a technique has been developed at IOZK to use blood serum-derived antigenic microparticles, where no fresh or frozen tumor tissue to produce a tumor lysate is available. This latter method was used in the case report above.
Thursday, 18 January 2018
Fluspirilene (schizophrenia drug)
Identification of antipsychotic drug fluspirilene as a potential anti-glioma stem cell drug
link to full study in Oncotarget
The TGS04 GBM glioma stem cell line used in the mouse study was established from a human glioblastoma at the University of Tokyo. These cells were implanted in the brains of nude mice. Fluspirilene was administered intramuscularly, as it is in humans.

Above: Fluspirilene treated mice had reduced tumor volume, increased survival and more sharply defined tumor borders (less diffuse).

Above: fluspirilene treated tumors showed greatly decreased expression of STAT3 with phosphorylation at serine 727. In other words, there was less activated STAT3 in these tumors.
"STAT3 can be transcriptionally activated by phosphorylation of its tyrosine 705 or serine 727 residue"
STAT3 is an important target in GBM and other cancers, helping to co-ordinate such cellular behaviours as invasion, angiogenesis, anti-apoptosis and immunosuppression.
link to full study in Oncotarget
The TGS04 GBM glioma stem cell line used in the mouse study was established from a human glioblastoma at the University of Tokyo. These cells were implanted in the brains of nude mice. Fluspirilene was administered intramuscularly, as it is in humans.

Above: Fluspirilene treated mice had reduced tumor volume, increased survival and more sharply defined tumor borders (less diffuse).

Above: fluspirilene treated tumors showed greatly decreased expression of STAT3 with phosphorylation at serine 727. In other words, there was less activated STAT3 in these tumors.
"STAT3 can be transcriptionally activated by phosphorylation of its tyrosine 705 or serine 727 residue"
STAT3 is an important target in GBM and other cancers, helping to co-ordinate such cellular behaviours as invasion, angiogenesis, anti-apoptosis and immunosuppression.
Wednesday, 17 January 2018
A difficult choice of treatment for a large progressive GBM after chemoradiotherapy
From some studies it follows that:
- Avastin in the first line increases the quality of life and survival for partially resected GBM;
- combination of CCNU + Avastin is more advantageous than just Avastin for MGMT-methylated GBM;
- I can not also not use TMZ immediately after chemoradiotherapy, especially after CeTeg results for MGMT-methylated GBM;
- low Avastin dose (<3.6 mg / kg / week) with Telmisartan, is more beneficial than the Avastin standard dose and will not be so toxic for use with CCNU + TMZ.
As a result, after sleepless nights, I decided to try this combination:
The cycle of 42 days:
0 day - Verapamil 240mg, Disulfiram 500mg, Copper 4mg, DHA 1200mg
1 day - Avastin 6.5 mg / kg
1 day - Lomustine 75 mg /m2 (+ Verapamil 240mg, Disulfiram 500mg, Copper 4mg, DHA 1200mg)
2-6 days - Temozolomide 90 mg/m2 (+ Verapamil 240mg, Disulfiram 500mg, Copper 4mg, DHA 1200mg, Curcumin 2000mg)
7-41 days - Telmisartan 40-80mg, Disulfiram 300mg, Copper 2mg, DHA 900mg)
15 day - Avastin 6.5mg / kg
29 day - Avastin 6.5mg / kg
42 day - Verapamil 240mg, Disulfiram 500mg, Copper 4mg, DHA 1200mg
+ every day Melatonin/Agomelatin, Berberin, Shark Oil, Oxaloacetate, Honokiol...
If possible, DCA will be added 6mg / kg / twice every day.
If possible, the doses of CCNU and TMZ in the next cycle will be increased.
- Avastin in the first line increases the quality of life and survival for partially resected GBM;
- combination of CCNU + Avastin is more advantageous than just Avastin for MGMT-methylated GBM;
- I can not also not use TMZ immediately after chemoradiotherapy, especially after CeTeg results for MGMT-methylated GBM;
- low Avastin dose (<3.6 mg / kg / week) with Telmisartan, is more beneficial than the Avastin standard dose and will not be so toxic for use with CCNU + TMZ.
As a result, after sleepless nights, I decided to try this combination:
The cycle of 42 days:
0 day - Verapamil 240mg, Disulfiram 500mg, Copper 4mg, DHA 1200mg
1 day - Avastin 6.5 mg / kg
1 day - Lomustine 75 mg /m2 (+ Verapamil 240mg, Disulfiram 500mg, Copper 4mg, DHA 1200mg)
2-6 days - Temozolomide 90 mg/m2 (+ Verapamil 240mg, Disulfiram 500mg, Copper 4mg, DHA 1200mg, Curcumin 2000mg)
7-41 days - Telmisartan 40-80mg, Disulfiram 300mg, Copper 2mg, DHA 900mg)
15 day - Avastin 6.5mg / kg
29 day - Avastin 6.5mg / kg
42 day - Verapamil 240mg, Disulfiram 500mg, Copper 4mg, DHA 1200mg
+ every day Melatonin/Agomelatin, Berberin, Shark Oil, Oxaloacetate, Honokiol...
If possible, DCA will be added 6mg / kg / twice every day.
If possible, the doses of CCNU and TMZ in the next cycle will be increased.
Histone deacetylase inhibitors (HDACi)
I find a lot of information that histone deacetylase inhibitors (Trichostatin A (TSA), Vorinostat, 7-ureido-N-hydroxyheptanamide derivative (CKD5)) have potent anti-cancer effects in glioblastoma.
2017 https://www.ncbi.nlm.nih.gov/pubmed/27852054
"Our results demonstrate that the novel HDACI CKD5 is a promising therapeutic candidate for glioblastoma."
2017 https://www.ncbi.nlm.nih.gov/pubmed/27766591
"We conclude that the combined administration of TSA and CCNU eradicates GBM cells with a higher efficacy than either drug alone, thereby opening a novel avenue for the treatment of GBM."
2015 https://www.ncbi.nlm.nih.gov/pubmed/25634603
"...these results indicate that trichostatin A (TSA) suppresses ESCC cell growth by inhibiting the activation of the PI3K/Akt and ERK1/2 pathways. TSA also promotes cell apoptosis through epigenetic regulation of the expression of apoptosis‑related protein."
2014 https://www.ncbi.nlm.nih.gov/pubmed/24464841
"Here, we investigate the effects of the HDACi trichostatin A (TSA) in U87 GBM cultures and tumorsphere-derived cells. These findings indicate that HDACis can inhibit proliferation, survival, and tumorsphere formation, and promote differentiation of U87 GBM cells, providing further evidence for the development of HDACis as potential therapeutics against GBM."
The results of clinical trials, however, did not give a good result:
Phase I/II Trial of Vorinostat Combined with Temozolomide and Radiation Therapy for Newly Diagnosed Glioblastoma: Final Results of Alliance N0874/ABTC 02.
2017 https://www.ncbi.nlm.nih.gov/pubmed/29016887
Phase II Study of Bevacizumab and Vorinostat for Patients with Recurrent World Health Organization Grade 4 Malignant Glioma.
2017 https://www.ncbi.nlm.nih.gov/pubmed/29133513
"Valproic acid has also recently been demonstrated to be a potent histone deacetylase inhibitor."
Many patients with glioblastoma take valproic acid (Depakote) against epileptic attacks. However, this has no effect on overall survival. Perhaps it is necessary to increase the dose or combination with something? I found that disulfiram increases the content of valproic acid in the blood.
And by the way, I can not find any medicine containing Trichostatin A.
2017 https://www.ncbi.nlm.nih.gov/pubmed/27852054
"Our results demonstrate that the novel HDACI CKD5 is a promising therapeutic candidate for glioblastoma."
2017 https://www.ncbi.nlm.nih.gov/pubmed/27766591
"We conclude that the combined administration of TSA and CCNU eradicates GBM cells with a higher efficacy than either drug alone, thereby opening a novel avenue for the treatment of GBM."
2015 https://www.ncbi.nlm.nih.gov/pubmed/25634603
"...these results indicate that trichostatin A (TSA) suppresses ESCC cell growth by inhibiting the activation of the PI3K/Akt and ERK1/2 pathways. TSA also promotes cell apoptosis through epigenetic regulation of the expression of apoptosis‑related protein."
2014 https://www.ncbi.nlm.nih.gov/pubmed/24464841
"Here, we investigate the effects of the HDACi trichostatin A (TSA) in U87 GBM cultures and tumorsphere-derived cells. These findings indicate that HDACis can inhibit proliferation, survival, and tumorsphere formation, and promote differentiation of U87 GBM cells, providing further evidence for the development of HDACis as potential therapeutics against GBM."
The results of clinical trials, however, did not give a good result:
Phase I/II Trial of Vorinostat Combined with Temozolomide and Radiation Therapy for Newly Diagnosed Glioblastoma: Final Results of Alliance N0874/ABTC 02.
2017 https://www.ncbi.nlm.nih.gov/pubmed/29016887
Phase II Study of Bevacizumab and Vorinostat for Patients with Recurrent World Health Organization Grade 4 Malignant Glioma.
2017 https://www.ncbi.nlm.nih.gov/pubmed/29133513
"Valproic acid has also recently been demonstrated to be a potent histone deacetylase inhibitor."
Many patients with glioblastoma take valproic acid (Depakote) against epileptic attacks. However, this has no effect on overall survival. Perhaps it is necessary to increase the dose or combination with something? I found that disulfiram increases the content of valproic acid in the blood.
And by the way, I can not find any medicine containing Trichostatin A.
Tuesday, 16 January 2018
One reason mouse studies don't translate to humans
I just came across a study that looked very interesting, showing increased survival in an orthotopic glioma mouse model when metformin is combined with temozolomide.
High-Dose Metformin Plus Temozolomide Shows Increased Anti-tumor Effects in Glioblastoma In Vitro and In Vivo Compared with Monotherapy
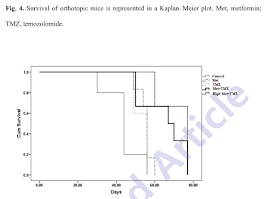


High-Dose Metformin Plus Temozolomide Shows Increased Anti-tumor Effects in Glioblastoma In Vitro and In Vivo Compared with Monotherapy
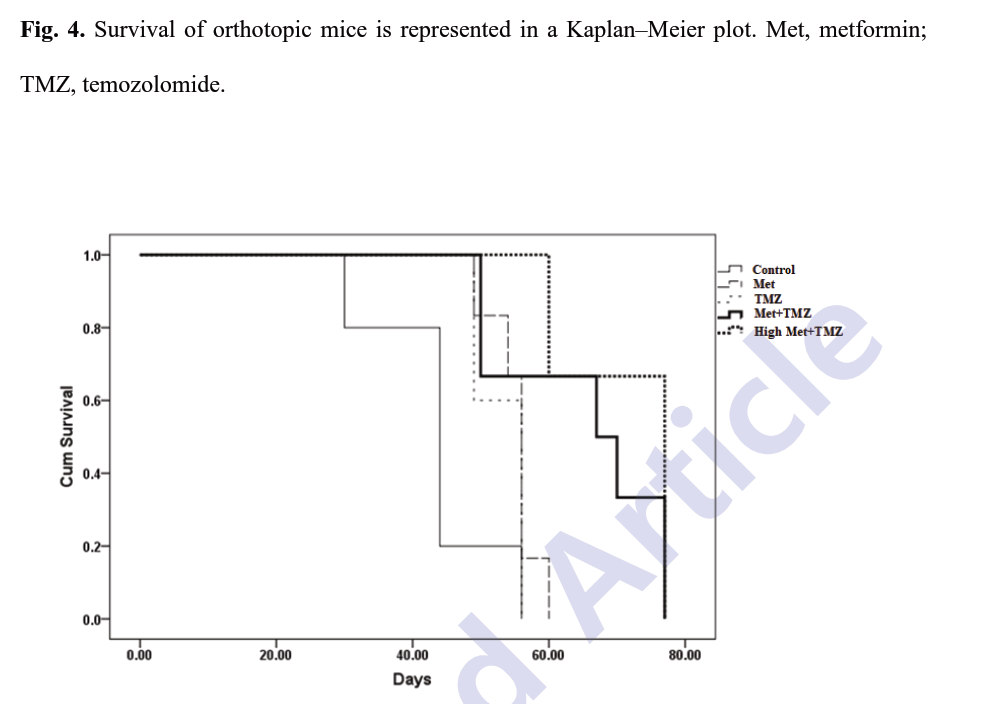
Especially interesting was the finding that the higher dose of metformin + temozolomide eliminated the expression of fatty acid synthase in the tumor specimens.

Fatty acid synthase (FASN) may be an especially good target in IDH1-mutant gliomas, as FASN is one of the most differentially overexpressed transcripts in G-CIMP (for the most part IDH mutant) gliomas versus non G-CIMP (for the most part IDH wild-type).

As is usually the case, the devil is in the details.
The study states several times that the metformin doses used in this study are clinically relevant, and this is true, except for the fact that the mice were injected with metformin intraperitoneally, rather than fed the metformin orally the way humans would take it.
From a different study, we know that intraperitoneal injections of metformin can lead to peak plasma levels 150-fold higher than what can be achieved with oral dosing.
"Notably, HPLC-ESI-QTOF-MS pharmacokinetic analysis showed that the plasma levels of metformin immediately after the last i.p. injection were ~150-fold higher than those obtained with the oral dosing schedule. Thus, mice that were treated with the i.p. dosing schedule achieved 679 ± 16 µmol/L (~87 µg/mL) metformin, a circulating dose of metformin that is within the lower limit observed in an individual with metformin poisoning..."
Pharmacokinetic differences between the methods of drug administration used in mouse studies (often intraperitoneal) and the methods used in humans, may account for some of the failures of mouse studies to translate into clinical results.
It would be interesting to investigate the anti-diabetes drug phenformin, a much more potent biguanide which was removed from the market in the 1970s due to increased risk of lactic acidosis, for cancer treatment.
Sunday, 14 January 2018
Lomustine or Axinitib? Phase 2 results.
Randomized phase II trial comparing axitinib with the combination of axitinib and lomustine in patients with recurrent glioblastoma.
https://www.ncbi.nlm.nih.gov/pubmed/28988341
https://static-content.springer.com/esm/art%3A10.1007%2Fs11060-017-2629-z/MediaObjects/11060_2017_2629_MOESM1_ESM.docx
Axitinib improves response rate and progression-free survival in patients with rGBM compared to historical controls. There is no indication that upfront combination of axitinib with CCNU improves results.
From this study does not follow that instead of Lomustin it is better to take Axitinib?
I need to decide what to add to Bevacizumab for my mom.
Saturday, 13 January 2018
CAR T THERAPY
Who are aware about Car T therapy?
http://time.com/4618566/brain-
Any clinics in Germany provide Car T therapy?
Thanks
http://time.com/4618566/brain-
Any clinics in Germany provide Car T therapy?
Thanks
Thursday, 11 January 2018
Avastin + Irinotecan?
It seems that my mother's tumor (MGMT methylated) did not decrease after radiation therapy + TMZ.
Doctors offer a combination Avastin + Irinotecan.
They say that if TMZ did not help by the time of radiotherapy, then TMZ will not even help with Lomustin!
But I have not seen a single message on this blog about Avastin + Irinotecan combination!
If we use it, what drugs do you recommend adding to increase efficiency?
Doctors offer a combination Avastin + Irinotecan.
They say that if TMZ did not help by the time of radiotherapy, then TMZ will not even help with Lomustin!
But I have not seen a single message on this blog about Avastin + Irinotecan combination!
If we use it, what drugs do you recommend adding to increase efficiency?
Wednesday, 10 January 2018
Anaplastic Astrocytoma questions
Hello,
First of all, thank you all for the time and work put into this site. I wish I had thought to look for it when my sister first got sick. This is the scariest stuff and it helps to see other families fighting and winning.
My sister was diagnosed with Astrocytoma 2 / 3 back in April 2016 which was determined to be Anaplastic Astrocytoma 3.
I don't understand what she meant but she said her tumor had "favorable" mutations.
She had 95% removal of the tumor at Sloan-Kettering, then moved on to radiation and chemo. She finished chemo in September(?) of last year.
All of her MRIs look good and her last one on 12/18/2017 was still clear.
My questions are:
1) Right now she is not really doing anything for maintenance. Would it be worth looking into a Ketogenic diet or meditation or anything? I would like to have her try the ketogenic diet, but I have read mixed things about it. Also, I want to push her to do this, but it's not my choice and it's hard to remember that.
2) I've read that Asctrocytoma conveys a huge risk to siblings and a lesser risk to parents. Would it be worth having my brother and parents get an MRI?
Thank you.
-Ray
Tactics of treatment for early continued growth.
10/27/2017 My mom had a surgical operation. Glyoblastoma was removed by 95%. (MGMT methylated)
After 3 weeks (11/16/2017) MRI showed that the tumor AGAIN grew to a size of 3.5 x 5 x 5 cm (accumulation of contrast medium)
Doctors were just shocked by such rapid growth!!!
From 21.11.2017 to 29.12.2017 my mother had radiation therapy + TMZ (+2 last weeks DCA, metformin, celebrex, chloroquine).
Now mom has a break. She accepts nothing. We want to restore blood counts. In addition, she had a terrible rash on her leg and on her arm.
Today's MRI showed continued growth. The size of the tumor is 4x5x6cm. (accumulation of contrast medium). Doctors say that this is not a pseudo-progression, since there is pressure on the brain and its displacement. We are at a loss.
Two weeks later, we wanted to start CCNU + TMZ (as in the CeTeG study) + DCA + rapamycin + hydroxy / chloroquine.
But now I'm not sure. Maybe we should start a daily low-dose TMZ + CUSPv4?
Or daily low-dose TMZ + DCA + rapamycin + hydroxy / chloroquine?
I'm afraid that my mother has little time. Her hand begins to work worse, she walks badly and does not speak well (
The tumor grows very quickly and I pray that we have a chance to try something.
Tuesday, 9 January 2018
Response to Optune imaged by amino acid PET
Amino Acid PET Imaging of the Early Metabolic Response During Tumor-Treating Fields (TTFields) Therapy in Recurrent Glioblastoma
I've uploaded this to the Brain Tumor Library (Optune/Novocure/NovoTTF folder)
Metformin in vivo, C6 glioma - Wistar rat model
This is the first study I've seen testing metformin in an orthotopic glioma model with oral (rather than intraperitoneal) administration. The survival gain was modest, but threre was a gain nonetheless.
http://exp-oncology.com.ua/wp/wp-content/uploads/2017/12/2419.pdf?upload= (see figure 4)
http://exp-oncology.com.ua/wp/wp-content/uploads/2017/12/2419.pdf?upload= (see figure 4)
Monday, 8 January 2018
Predicting immunotherapy response
1. The company OncoDNA provides test OncoDeep: 70 genes + predicting immunotherapy response.
https://www.oncodna.com/en/immunotherapy/
Price: 2990Eur.
Are there any studies predict immune therapy in other laboratories? Is this study useful?




3. Here (https://www.cegat.de/en/diagnostics/tumor-diagnostics/ovarian-cancer/) it is reported that "The detection of a somatic or germline mutation in the BRCA1 or BRCA2 genes is a requirement for treatment with Olaparib (LynparzaTM)"
There are also 4 testing options.
"Option 1: BRCA1 and BRCA2 analysis in tumor tissue only
In option 1, only mutations in the tumor are analyzed, no differentiation between germline and somatic mutations can be made. We do not recommend this option, but will perform it when it is explicitly requested by a patient."
Is it necessary to do such a study to determine the possibility of treatment with Olaparib or is it enough to study Oncodeep (by OncoDNA)? But in Oncodeep only mutations in the tumor are analyzed.
Option 1: BRCA1 and BRCA2 analysis in tumor tissue only
 Option 4: Somatic Tumor Panel
Option 4: Somatic Tumor Panel

https://www.oncodna.com/en/immunotherapy/
Price: 2990Eur.
Are there any studies predict immune therapy in other laboratories? Is this study useful?



2. By the way, in Moscow (Russia) a study of 50 genes costs $480. Can this research give some useful information? Or these 50 genes is very limited and such information is not sufficient?
3. Here (https://www.cegat.de/en/diagnostics/tumor-diagnostics/ovarian-cancer/) it is reported that "The detection of a somatic or germline mutation in the BRCA1 or BRCA2 genes is a requirement for treatment with Olaparib (LynparzaTM)"
There are also 4 testing options.
"Option 1: BRCA1 and BRCA2 analysis in tumor tissue only
In option 1, only mutations in the tumor are analyzed, no differentiation between germline and somatic mutations can be made. We do not recommend this option, but will perform it when it is explicitly requested by a patient."
Is it necessary to do such a study to determine the possibility of treatment with Olaparib or is it enough to study Oncodeep (by OncoDNA)? But in Oncodeep only mutations in the tumor are analyzed.
Option 1: BRCA1 and BRCA2 analysis in tumor tissue only


Saturday, 6 January 2018
Consequences of radiation therapy?
Please share your experience.
A week ago, my mother finished radiation therapy + temolozolomide.
The condition was good.
Now she has great weakness, all the time very sleepy, it's hard to walk, sometimes unnatural speech.
I can not understand, such weakness is the consequences of radiation therapy?
Also the last 2 weeks my mom takes every day Metformin (2х1000mg), DCA (2х1300mg), delagil (1х250mg), celebrex (2х200mg).
P.S. My mother also had a very low leukocyte count to 1.66 (norm 4.5-11). What do you recommend food additives for their increase?
A week ago, my mother finished radiation therapy + temolozolomide.
The condition was good.
Now she has great weakness, all the time very sleepy, it's hard to walk, sometimes unnatural speech.
I can not understand, such weakness is the consequences of radiation therapy?
Also the last 2 weeks my mom takes every day Metformin (2х1000mg), DCA (2х1300mg), delagil (1х250mg), celebrex (2х200mg).
P.S. My mother also had a very low leukocyte count to 1.66 (norm 4.5-11). What do you recommend food additives for their increase?
Thursday, 4 January 2018
First post- looking for advice on cocktail treatment
Hello,
This is my first time posting to this site, although I have come across it many times in my research. My name is Jenna and I am here on behalf of my father who was diagnosed at age 66 and will turn 68 this February. Although his tumor is currently stable, his symptoms appear to be worsening. He has increased confusion and sleeps on and off all day. I am here looking for some suggestions as to what we do next.
A brief history: my father was diagnosed with grade 4 GBM in August 2015 and had a successful resection on his right frontal lobe and started temozolomide and radiation treatment. We tested the tumor material with FoundationOne and found six genomic alternations: EGFR, PIK3CA, CDKN2A/B, FAT1, and TERT. We also learned that it was unmethylated. His first recurrence was in September 2016, again in the right frontal lobe. We decided to try the Tocagen immunotherapy study, but unfortunately in late March, we saw growth again in the right frontal lobe as well as new growth in the corpus callosum, making it inoperable. Since then, my dad started getting infusions of nivolumab with re-radiation and we’ve been getting scans that show a slight improvement which has given us a few small but welcome moments of relief. At the same time, the re-radiation or nivo have caused inflammation and we believed the added pressure from that was giving him balance and bladder control issues. He recently had a seizure and now we are trying to work out whether his balance issues were actually the results of something called Todd's Paralysis. It's possible he's been having several small seizures that have been going unnoticed which then cause weakness in the limbs for days to months. If this is the case, we might be able to decrease or remove the steroids. We also reduced his nivolumab infusions from every two weeks to once a month to see if it lessens his inflammation.
I read Ben Williams' book as well as some posts here about cocktail treatments. I would love to create a regimen for my Dad but am confused about where to start. I work in anti-counterfeiting as well which makes me extra wary about procuring drugs from the internet. I would love to hear from some of you about which combinations of treatments are working, where the agents can be safely obtained, what the dosage is, and whether or not there are any side effects.
Many thanks and wishing everyone a happy new year ahead!
Jenna
Tuesday, 2 January 2018
P53 loss questions
Hi all,
I'm in the middle of determining what my next steps will be following my AA3 (previously thought to be an Oligo 2) diagnoses.
The tumour is listed as having P53 loss (or truncated mutation), which I know is more unusual in this type of tumour. While doing research on a ketogenic diet I repeatedly came across brief descriptions of p53 playing a role in metobolism...so I decided to look into it more. Below are a few links to different papers I've read. It's seems like you can exploit this loss in a number of different ways.
Firstly, there is evidence that it has some role in fatty acid oxidation and glutathione oxidation (I do not have a mutation to the MYC gene - which also plays a role in glutathione oxidation). According to these papers, these tumours (with p53 loss) are highly vulnerable to glucose restriction, they allow the PPP to become unchecked - which is a pathway that metabolises glucose. (I have read that p53 loss may prevent gene mutations (I think I was understanding that right), which maybe why I do not have an MYC mutation (the mutations I do have are listed in my post called Pathology Report from a few weeks ago).
It also regulates ROS homeostatsis, either through pro or anti-oxidant means (would loss of p53 mean that ROS was unchecked and how would this impact IDH1 mutant gliomas where ROS is already significantly altered, right?) In general, I'm questioning how IDH1 mutation works with loss of p53? IDH mutation metabolises glutamate at high rates, correct? So if p53 is lost (therefore the tumour would not generate GLS2 (at least through P53) and I do not have an MYC mutation (which allows the tumour to uptake large amounts of GLS1 - both GLS1 and 2 metabolise glutathione, then what others ways what the cells use glutathione?
I'm also questioning whether a ketogenic diet would be useful if I am able to use Proton therapy. I believe all radiation therapy uses ROS as one mechanism, proton therapy using more. A ketogenic diet has been said to limit ROS (sort of like antioxidants) but if it will limited it in standard therapy will more be better in Proton therapy? And then, the P53 in relationship to ROS question also comes in here.
I have read that keto may not be good for an IDH mutant tumour because of NAD+. Can someone elaborate more on that?
Just some more info - I had a gross total resection (surgeon said 99.9%). I'm considering Proton Therapy (do people have a hard time getting that covered by insurance), CBD/THC is try to block glutathione uptake during radiation, ketogenic diet to block glucose with attention to glutamate and methionine intake and DHC fatty acids, if needed boswellia and celebrex to prevent need for steroids, Stephen has recommended disulfiram, which I will look into and I'm going to look into metformin (seems to have a special interest with P53 loss), curcumin ( I was taking it before surgery) and I'm considering not taking any chemo at this time.
I apologize that I'm not as organized as I could be in asking these questions. I am experiencing aphasia following surgery.
Here are the links:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3135642/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2763495/
http://www.pnas.org/content/107/16/7117.full
http://www.sciencedirect.com/science/article/pii/S0005272809000115
https://www.ncbi.nlm.nih.gov/m/pubmed/21336310/
Thank you all.
Maria
I'm in the middle of determining what my next steps will be following my AA3 (previously thought to be an Oligo 2) diagnoses.
The tumour is listed as having P53 loss (or truncated mutation), which I know is more unusual in this type of tumour. While doing research on a ketogenic diet I repeatedly came across brief descriptions of p53 playing a role in metobolism...so I decided to look into it more. Below are a few links to different papers I've read. It's seems like you can exploit this loss in a number of different ways.
Firstly, there is evidence that it has some role in fatty acid oxidation and glutathione oxidation (I do not have a mutation to the MYC gene - which also plays a role in glutathione oxidation). According to these papers, these tumours (with p53 loss) are highly vulnerable to glucose restriction, they allow the PPP to become unchecked - which is a pathway that metabolises glucose. (I have read that p53 loss may prevent gene mutations (I think I was understanding that right), which maybe why I do not have an MYC mutation (the mutations I do have are listed in my post called Pathology Report from a few weeks ago).
It also regulates ROS homeostatsis, either through pro or anti-oxidant means (would loss of p53 mean that ROS was unchecked and how would this impact IDH1 mutant gliomas where ROS is already significantly altered, right?) In general, I'm questioning how IDH1 mutation works with loss of p53? IDH mutation metabolises glutamate at high rates, correct? So if p53 is lost (therefore the tumour would not generate GLS2 (at least through P53) and I do not have an MYC mutation (which allows the tumour to uptake large amounts of GLS1 - both GLS1 and 2 metabolise glutathione, then what others ways what the cells use glutathione?
I'm also questioning whether a ketogenic diet would be useful if I am able to use Proton therapy. I believe all radiation therapy uses ROS as one mechanism, proton therapy using more. A ketogenic diet has been said to limit ROS (sort of like antioxidants) but if it will limited it in standard therapy will more be better in Proton therapy? And then, the P53 in relationship to ROS question also comes in here.
I have read that keto may not be good for an IDH mutant tumour because of NAD+. Can someone elaborate more on that?
Just some more info - I had a gross total resection (surgeon said 99.9%). I'm considering Proton Therapy (do people have a hard time getting that covered by insurance), CBD/THC is try to block glutathione uptake during radiation, ketogenic diet to block glucose with attention to glutamate and methionine intake and DHC fatty acids, if needed boswellia and celebrex to prevent need for steroids, Stephen has recommended disulfiram, which I will look into and I'm going to look into metformin (seems to have a special interest with P53 loss), curcumin ( I was taking it before surgery) and I'm considering not taking any chemo at this time.
I apologize that I'm not as organized as I could be in asking these questions. I am experiencing aphasia following surgery.
Here are the links:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3135642/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2763495/
http://www.pnas.org/content/107/16/7117.full
http://www.sciencedirect.com/science/article/pii/S0005272809000115
https://www.ncbi.nlm.nih.gov/m/pubmed/21336310/
Thank you all.
Maria
Monday, 1 January 2018
Drug for a cocktail before bedtime?
Melatonin, agomelatin, imipramine, amitriptyline or something different?
As I can see, many patients take 20mg of melatonin before bedtime.
However, as written in CUSPND
"Agomelatine’s circulating half-life in humans is ~2hours versus 30 to 40 minutes for melatonin. This is a significant advantage of agomelatine. Further complicating the use of melatonin would be the variable and generally poor absorption after oral administration. Agomelatine penetrates the blood-brain barrier."
This study (https://www.ncbi.nlm.nih.gov/pubmed/28500556) compared agomelatine and other drugs and concluded that the most effective for glioblastoma - imipramine or amitriptyline.
However, here (https://www.ncbi.nlm.nih.gov/pubmed/27480195) on the contrary it is reported "that imipramine and tranylcypromine reduced the cytotoxic efficacy of temozolomide under some oxygen conditions while fluoxetine did not demonstrate such effects".
So which of these drugs should be added to the cocktail before bedtime?
CLOVA cocktail - Your opinion?
It was published in February 2017:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5410264/
"The patients treated with CLOVA cocktail in combination with TMZ showed increased survival compared to the control group treated with TMZ alone."
CLOVA cocktail:
TMZ + 800 mg cimetidine, 400 mg lithium, 10 mg olanzapine, 800 mg valproate.
Perhaps one of these drugs (to inhibit the activity of GSK3β) can be replaced with more effective?