Hello all,
I found this trial in Europe (Heidelberg Germany):
https://clinicaltrials.gov/show/NCT02718443
http://abstracts.asco.org/199/AbstView_199_191829.html
What's your opinion, does it seem something that could work on recurrent AA3 (IDH1 mutated, MGMT methylated) (ASCO abstract goes beyond my understanding... :)
Or would it be better to go with PARP + TMZ combo?
br,
Juha
Sunday, 30 July 2017
Saturday, 29 July 2017
Levi's cocktail
Stephen, and dear blog visitors, I'd also be grateful if you could review my husband's not so extensive cocktail. Should I increase the dosages or should I add something to the list in your opinion?
I'm so desperate to help him defeat this nasty disease. I know that I'm too hesitant and that we don't have time for that. My husband was shocked about his diagnose so he don't want to read about the possible treatments and drugs so everything is on my shoulders. I totally understand his attitude although it would be such a great help if he would be proactive because he is the smartest person I've ever met. His NO is a very good professional but absolutely not on board, just SOC. We don't even have the courage to ask for his opinion.
Unfortunately we started the majority of these drugs only after radiochemotherapy (except of Metformin and alfacalcidol). We added Aciclovir and CQ on the last week of the radiation therapy. Fluoxetin and DCA right after the last day of RT. Celebrex only 2 weeks ago.
He weighs 70 kg (ca. 154 pounds) if it matters.
Official:
Medrol 16 mg (chorticosteroid - in Hungary we don't have Decadron) This is one tablet only and I'd like to reduce it by half because we have Celebrex but my husband is hesitant because we only have appointment to the NO on 21/8. He has no symptoms other than extreme fatigue and metallic taste in his mouth.
Prescription drugs:
- Metformin - we recently increased it from 850 mg to 1275 mg (This is 1.5 tablet)
- Chloroquine 250 mg
- Fluoxetin 20 mg (Should we increase it to 40 mg? He is quite depressed even after more than a month on it so it just would be a bonus if his mood would be better.)
- Celebrex 200 mg x 2
- DCA 500 mg x 2 on a 2 week on 1 week off basis. We'd like to increase it to 500 mg x 3 as soon as he finishes his first TMZ cycle. Up until now he has not experienced neuropathy although he takes 1 pill of Milgamma Neuro every other day which contains 40 mg of benfothiamin, 90 mg B6 and 0,25 mg B12. We use the product of DCA Lab.
- alfacalcidol 2,5 mcg
Around chemo days:
- Aciclovir 400 mg x 2 (I'm just guessing what would be the right dosage and maybe he should take it daily, not only around TMZ days.)
- Omeprazole 40 mg x 2
His Canadian friend will bring him cimetidine within a few weeks. I'd like him to take 1000 mg a day.
I've just read about clomipramine here but I suppose that you can't use clomipramine and fluoxetin together. Which one has more benefit in your opinion? Mouse evidence on one hand and lots of anecdotal success stories on the other hand.
My husband never had a seizure so I'm hesitant to give him Keppra although its chemosensitizing properties are very tempting.
I have propranolol and I'm thinking to start my husband on it after the first MRI but I'm afraid to mess with his blood pressure. Based on the etodolac + propranolol trial I hope it can be effective with the standard 5/23 protocol, too. I'm assuming that Celebrex can be an appropriate alternative to etodolac.
Although we have a good relationship with our GP who is helpful enough to prescribe for us the above mentioned drugs, I think that she would be reluctant to prescribe tamoxifen, disulfiram, minocycline or maybe even mebendazole on the long term. What do you think of such providers like Alldaychemist? Is it risky to buy from them? Any personal experience?They even have Valcyte which I haven't been able to convince anybody to prescribe since my husband is seronegative for CMV. He had it once but now he has no active CMV infection.
Non-prescription:
- Genistein (Soy Isoflavones) 28 mg x 2 (We are not so convinced about it and my husband hates it so I think I'm not going to buy it again.)
- Silibinin 86,5 mg x 6
- melatonin 20 mg
- ca. 1 dl / 3 oz (?) frozen breast milk except of TMZ days (I know, I know...but it was easy to get it through a reliable relative.)
- propolis (30 drops)
- 1 liter green tea on TMZ days with Omega 3 and 200 mg ascorbic acid
- 1 teaspoon of home-made ethanolic rosehip tincture daily (except of TMZ days) because of this study http://www.scirp.org/
I know Stephen what you think about in vitro results but it's so easy to make and it can't do harm.
During RT he ate tons of lycopene-rich tomato juices and home made rosehip puree and steamed broccoli and broccoli sprouts because of sulforaphane. The latter now he hates so he'll start soon on broccoli sprout capsules. I also give him fresh pomegranate juice almost every day.
As you can see we are not so eager about supplements, they seem a bit unproven for us but I recently ordered Longvida curcumin (although its poor bioavailability), liquid Maitake D fraction, Selenium and CQ10.
Is CQ10 and Selenium applicable in between TMZ cycles despite their strong antioxidant properties?
Also, we tried a popular Hungarian medicinal mushroom complex (8 pills contain 150 mg rezveratrol, 336 mg shiitake, 336 mg ganoderma, 336 mg maitake, 336 mg almond mushroom) but he had severe diarrhea even on 2 pills a day so I'm not so confident to order him the Mushroom Science PSK product that everyone uses. I didn't see anybody encountering this problem on any cancer forum. It would be a pity to miss it.
I bought some edible oregano essential oil because of these articles but we don't know how to administer it. First, he tried to dissolve 5 drops under his tongue but it has awful taste. Later he tried to drink 5 drops with water. It's also a very strong antioxidant so maybe it's not so smart decision to use it when he is on DCA. or in between chemo cycles.
https://www.linkedin.com/pulse/oregano-compound-activates-oocytes-kills-glioblastoma-finley
https://www.ncbi.nlm.nih.gov/pubmed/25965832
We'd like to obtain 1:1 THC-CBD oil, too. Could you please provide me with some reliable resources? A lot of people seem to take it but I don't know where to buy it.
Big thank you to Stephen and this helpful community.
GBM treatment options with a moderate budget
My 29 years old husband was diagnosed on 3/26 with a multifocal, thalamic GBM. We are from Hungary. He has undergone surgery on the 5th of April. 80% of the walnut-sized tumor was resected from his thalamus. His other, frontomediobasal tumor seems to be inactive (although it's pretty big, too) so the surgeon didn't resect it and it didn't received radiation either. He has completed SOC and currently is on his first cycle of 5/23 TMZ monotherapy. He has no EGFR amplification. His tumor is IDH negative and indeed very aggressive. Only 3 weeks after surgery he was hospitalized because of edema which was caused by tumor regrowth. So now he has quite a few smaller tumors around his thalamus besides the remaining 20% piece.
His first post-radiation MR is scheduled for the middle of August. Since I've not yet received the information regarding his MGMT methylation status (long story) I'm constantly worrying and seeking for opportunities in case of tumor progression since in my country there's no protocol for recurrent glioblastoma other than Avastin. I mean no PCV or other chemos, no immunotherapy, no clinical trials, no Optune device (I requested an offer from Germany and it turns out that it costs 30 000 € /months and you need a technical and medical support at home).
I'm aware that we need to manage our finances cleverly in this situation. If you had up to 20,000-30,000 USD which option or options would you go for?
- Immunotherapy in Germany (It seems to me that only Nesselhut Clinic fits into our budget but reviews are not so convincing as nothing in the world of GBM.)
- Keytruda / Opdivo immunotherapy + TMZ
In Hungary it's not part of the protocol but hopefully we can find a doctor who will prescribe it at our own expense. As I can see Opdivo has kind of failed; is Keytruda. better? Do we need PD-L1 testing to get it?
- We have gamma knife in Hungary and it can be paid through National Insurance (so patients who qualify don't need to pay for it) but doctors are reluctant to let GBM patients to choose this option. It's usually used for small and simple tumors and for brain metastases. If our NO will advise against it or will be not so eager to help maybe I can search for other European gamma knife possibilities although I can't find too many comments on gamma knife and GBM.
- Neuroblate Laser Ablation. As far as I know it's exactly for problematic tumors, like thalamic ones. I'm planning to send them an inquiry but I have concerns about whether it is an adequate alternative to surgery for inoperable tumors. Can it prolong life or is it just a palliative treatment? How much would be the estimated cost? Has anybody personal experiences with it? Is laser ablation superior to gamma knife?
Our NO said my husband's thalamic tumor is no accessible for surgery anymore and considering his bad reaction to the first surgery maybe laser ablation or gamma knife wouldn't be the best option for him. What are your thoughts on it?
- SPMF treatment in India. It's quite cheap but no statistics are available and it's so hard to believe for me that the same effect is achievable with 1-2 hours of treatment for 28 days as with the Optune cap which you need to wear almost all day long up until it works. I've read about a young patient with thalamic tumor on Inspire who had Optune and it didn't do any good for him because of the location. I suppose that the same applies for SPMF, too.
- I sent an inquiry to Duke's polio virus trial.
My clinical trial applications have been ignored from all over the world so I was tricky enough to mention that "I'm aware that non-U.S. citizens should cover their costs on their own in case of qualifying for a clinical trial and I hope I can manage it with the help of my family. "
I got this answer from doctor Friedman personally "We would not have a trial for you at this time since the surgery was so long ago and the tumor is not growing If it ever does regrow please let us know"
Maybe it was just a polite "no" or maybe this possibility is truly open for us in case of a recurrence but the truth is that I have no idea how much a treatment like this could cost in one of the world's best institutions for cancer. Anybody has any idea about their fees?
- Ask the Brazilian doctor to come to Hungary and teach us to administer Perillyl Alcohol. I've read that the brave persons who tried to make it themselves found it unbearable to use.
Any and all help is very much appreciated. Thank you in advance and sorry for my grammar mistakes.
PARP combination therapy
Hello all,
I came across this article:
http://dx.doi.org/10.1016/j.critrevonc.2016.10.010
Does someone have experience regarding PARP combination therapy? I know this has been discussed before in other posts especially when a tumour is IDH1-mutated. In the article they also propose that MGMT methylation is positive factor for PARP therapy.
It would be interesting to see results from trials or hear personal experiences on PARP therapy.
All the best,
Juha
I came across this article:
PARP inhibitor combination therapy
"Here, we summarise both the pre-clinical and clinical evidence for the utility of such combinations and discuss the future prospects and challenges for PARP inhibitor combinatorial therapies."http://dx.doi.org/10.1016/j.critrevonc.2016.10.010
Does someone have experience regarding PARP combination therapy? I know this has been discussed before in other posts especially when a tumour is IDH1-mutated. In the article they also propose that MGMT methylation is positive factor for PARP therapy.
It would be interesting to see results from trials or hear personal experiences on PARP therapy.
All the best,
Juha
Tuesday, 25 July 2017
Kudos and Hindsight's 20/20 Thoughts
I lost my dear husband after 32 years of marriage to a GBM that his
colleagues at MD Anderson recognized as so genetically virulent, they
did not give him more than a few months, at most, after diagnosis. I
will never forget sitting in a room, surrounded by the large group of
oncologists who were his close friends, waiting on the results and then
seeing them cry as his case was discussed.
Against their wishes, we started him on a course of supplements to accompany the chemo and radiation. It included pycnogenol, cannabis oil, curcumin, Leukozepin, Vit. D, turkey tail mushrooms, boswellia, artemisinin, and more, plus organic smoothies. He had 2-3 acupuncture treatments per week. It caused an uproar. He was a traitor to modern science. Every consult was a battle. Didn't we realize that free radicals were our FRIENDS?? And we would answer back our retort, and they would argue back theirs. It was awful...the whole experience was a nightmare because he dared to think outside the box and at MD Anderson's Dept. of Neuro-oncology, that is a sin. There were times the pressure was so great, he actually stopped the supplements for awhile, or stopped some of them. And did it help? No. The tumor took advantage of the "rest" it got and grew even faster. So he'd go back on them, having lost ground.
He was even ok'd for a clinical trial as n-of-1, with the supplements having been ok'd by the principal investigator, but the head of the NO department said that no one would go on any trial in his department as long as the patient took supplements, not even a pre-approved n-of-1. The fact that my husband had been a researcher "in the family" for 30 years, who had done his due diligence, and made the decision to go forward, meant nothing. And as the department head made this proclamation, he smiled a Mona Lisa smile that said, "It doesn't matter, you know, you are going to die before long anyway."
It is something I will never forgive.
My husband lived almost a year after his diagnosis, to the surprise of all who knew his profile. And in the last few months, I have relived every decision we made along the way. May I share my hindsight with you? Who knows, it might help someone.
1. First of all, kudos to Stephen and the rest of you, for asking so many questions and thinking of novels ways to attack this monster. If the NOs won't think outside the box for all of the insurance/funding/politics/training/messy-science/too-many-variables reasons, then we are on our own. Keep it up. This is a glioblastoma...time for a new paradigm, folks.
2. If we had to do it all over again, he'd have gone through the resection, but not the radiation. The only thing the radiation did was to make the beast bigger. Yes, it was floppy and full of holes. But it was MGMT-promoter gene unmethylated. That radiation + Temodar just kicked it in the shins a little. When that -blastoma beast regained its strength and got back to the business of evolving, it handily filled in those holes and started to grow again with newer, more efficient angiogenic pathways, but now starting from the larger border! And with each new chemo agent, it created another new angiogenic pathway that was even better than the one before. In what universe is this a good idea?
3. We would have started him on all of his supplements, immediately after the resection, especially cannabis. You can get it, you just have to try. Go to the Facebook GBM cannabis blog and put it out there...hey! I'm in an illegal state! Help me, please??? and you will be helped. But get someone to tell you how to dose it. We were conservative Repubs at the time and didn't know the first thing about CO. We finally consulted, via FaceTime, with Eloise at Green Health Consultants and she did her best but it was too little too late.
4. Start on Optune when the tumor is small, not when it is really big like we did. In Houston, you will have to go to Methodist Hospital to do this. Husband's new NO, Dr. Ivo Tremont-Lukats, was trained at MD Anderson and is willing to let you use whatever supplements you want. He's a gem.
5. Because Husband's tumor's MGMT-promoter gene was unmethylated, we would have gotten him on disulfiram asap, to take along with the Temodar. I did get some on the black market about mid-way through but it arrived two years out of date. Dr. Tremont was willing to let my husband have a Hail-Mary trial of it toward the end, but by then the tumor had covered most of his brain and was creeping down his spine. Like I said, it was especially virulent. Had his NO at MD Anderson been willing to write a legitimate RX for it after the resection, when that puppy was the size of a peanut, I really think my husband might've had a chance to stop, or at least slow down, its regrowth. And every time he took Temodar after that, he would have needed to take the disulfiram at the same time. That, along with the carpet bomb effect of the supplements and Optune, would have given him better odds than what we were dealt at MD Anderson, I'm convinced.
That's it. That's all I have to offer. My rage at the medical establishment is something I will be working on for a long time. I have a couple wonderful of "forgiveness" counselors who are helping me with this via phone sessions and I am slowly getting better, I think.
Best of luck to you and may our Lord bless you and keep you in His hands.
Against their wishes, we started him on a course of supplements to accompany the chemo and radiation. It included pycnogenol, cannabis oil, curcumin, Leukozepin, Vit. D, turkey tail mushrooms, boswellia, artemisinin, and more, plus organic smoothies. He had 2-3 acupuncture treatments per week. It caused an uproar. He was a traitor to modern science. Every consult was a battle. Didn't we realize that free radicals were our FRIENDS?? And we would answer back our retort, and they would argue back theirs. It was awful...the whole experience was a nightmare because he dared to think outside the box and at MD Anderson's Dept. of Neuro-oncology, that is a sin. There were times the pressure was so great, he actually stopped the supplements for awhile, or stopped some of them. And did it help? No. The tumor took advantage of the "rest" it got and grew even faster. So he'd go back on them, having lost ground.
He was even ok'd for a clinical trial as n-of-1, with the supplements having been ok'd by the principal investigator, but the head of the NO department said that no one would go on any trial in his department as long as the patient took supplements, not even a pre-approved n-of-1. The fact that my husband had been a researcher "in the family" for 30 years, who had done his due diligence, and made the decision to go forward, meant nothing. And as the department head made this proclamation, he smiled a Mona Lisa smile that said, "It doesn't matter, you know, you are going to die before long anyway."
It is something I will never forgive.
My husband lived almost a year after his diagnosis, to the surprise of all who knew his profile. And in the last few months, I have relived every decision we made along the way. May I share my hindsight with you? Who knows, it might help someone.
1. First of all, kudos to Stephen and the rest of you, for asking so many questions and thinking of novels ways to attack this monster. If the NOs won't think outside the box for all of the insurance/funding/politics/training/messy-science/too-many-variables reasons, then we are on our own. Keep it up. This is a glioblastoma...time for a new paradigm, folks.
2. If we had to do it all over again, he'd have gone through the resection, but not the radiation. The only thing the radiation did was to make the beast bigger. Yes, it was floppy and full of holes. But it was MGMT-promoter gene unmethylated. That radiation + Temodar just kicked it in the shins a little. When that -blastoma beast regained its strength and got back to the business of evolving, it handily filled in those holes and started to grow again with newer, more efficient angiogenic pathways, but now starting from the larger border! And with each new chemo agent, it created another new angiogenic pathway that was even better than the one before. In what universe is this a good idea?
3. We would have started him on all of his supplements, immediately after the resection, especially cannabis. You can get it, you just have to try. Go to the Facebook GBM cannabis blog and put it out there...hey! I'm in an illegal state! Help me, please??? and you will be helped. But get someone to tell you how to dose it. We were conservative Repubs at the time and didn't know the first thing about CO. We finally consulted, via FaceTime, with Eloise at Green Health Consultants and she did her best but it was too little too late.
4. Start on Optune when the tumor is small, not when it is really big like we did. In Houston, you will have to go to Methodist Hospital to do this. Husband's new NO, Dr. Ivo Tremont-Lukats, was trained at MD Anderson and is willing to let you use whatever supplements you want. He's a gem.
5. Because Husband's tumor's MGMT-promoter gene was unmethylated, we would have gotten him on disulfiram asap, to take along with the Temodar. I did get some on the black market about mid-way through but it arrived two years out of date. Dr. Tremont was willing to let my husband have a Hail-Mary trial of it toward the end, but by then the tumor had covered most of his brain and was creeping down his spine. Like I said, it was especially virulent. Had his NO at MD Anderson been willing to write a legitimate RX for it after the resection, when that puppy was the size of a peanut, I really think my husband might've had a chance to stop, or at least slow down, its regrowth. And every time he took Temodar after that, he would have needed to take the disulfiram at the same time. That, along with the carpet bomb effect of the supplements and Optune, would have given him better odds than what we were dealt at MD Anderson, I'm convinced.
That's it. That's all I have to offer. My rage at the medical establishment is something I will be working on for a long time. I have a couple wonderful of "forgiveness" counselors who are helping me with this via phone sessions and I am slowly getting better, I think.
Best of luck to you and may our Lord bless you and keep you in His hands.
Simvastatin positive evidence in an orthotopic GBM model
The study is called MYC-regulated Mevalonate Metabolism Maintains Brain Tumor Initiating Cells


This study constitutes in my view the first solid evidence that statins could be useful in GBM therapy. In accordance with my research, simvastatin was the statin selected which has better blood-brain barrier abilities versus some other statins, for example atorvastatin (see figure below). The drug in this study was injected intraperitoneally rather than given orally as would be the case in humans, but at least they used a brain-implanted (not subcutaneous flank-injected) model with relatively recently created GBM cell lines (rather than the ancient U87).
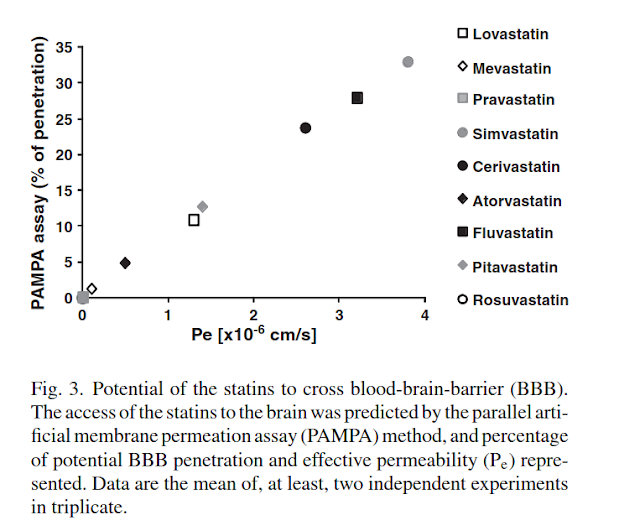
Figure above from the study Statins as Neuroprotectants: A Comparative In Vitro Study of Lipophilicity, Blood-Brain-Barrier Penetration, Lowering of Brain Cholesterol, and Decrease of Neuron Cell Death by Sierra et al. Journal of Alzheimer’s Disease 23 (2011) 307–318.


This study constitutes in my view the first solid evidence that statins could be useful in GBM therapy. In accordance with my research, simvastatin was the statin selected which has better blood-brain barrier abilities versus some other statins, for example atorvastatin (see figure below). The drug in this study was injected intraperitoneally rather than given orally as would be the case in humans, but at least they used a brain-implanted (not subcutaneous flank-injected) model with relatively recently created GBM cell lines (rather than the ancient U87).

Figure above from the study Statins as Neuroprotectants: A Comparative In Vitro Study of Lipophilicity, Blood-Brain-Barrier Penetration, Lowering of Brain Cholesterol, and Decrease of Neuron Cell Death by Sierra et al. Journal of Alzheimer’s Disease 23 (2011) 307–318.
ONC 201 or Avastin?
Stephen and all,
We are trying to decide between treating our son (recurrent glioma, H3 K27 mutant, mutations in ASXL 1 and PIK3CA among others) with Avastin +Irotican or the new ONC201 trial. We tend to think that ONC201 is a better option. What do you think? Thanks!
We are trying to decide between treating our son (recurrent glioma, H3 K27 mutant, mutations in ASXL 1 and PIK3CA among others) with Avastin +Irotican or the new ONC201 trial. We tend to think that ONC201 is a better option. What do you think? Thanks!
Sunday, 23 July 2017
posts on DCA from the old cancer compass thread
I found some of the discussions on the old cocktails thread at cancer compass concerning DCA useful, including the two below.
April 19, 2015:
May 16, 2015
April 19, 2015:
I talked with three different suppliers and one Canadian pharmacy about purchasing DCA. One company was rude, would not address my questions, and worse. Very evasive in who they were and quality issues. My selection came down to two providers and ultimately I went with pharma-dca. I chose this company because they claim their DCA is manufactured in the UK, not china like almost all other DCA. They addressed my questions respectfully and I liked one of the responses I received from them (see below). Additionally I was looking for someone else that had sourced their DCA through pharma-dca and found that Cheryl Broyles does.
Caveat emptor seems like a very important precaution here. I have not had their DCA independently tested. Therefore it could be excellent quality, it could be adulterated or not DCA at all. I am in no way suggesting their product is not what they claim, I am simply saying I have not had it tested. In my conversations with others using DCA, some source their product through pharma-dca as well and have no complaints. By the way, the other source I was inclined to trust was Certified DCA, but they were asking quite a bit more for their DCA. Below is pharma DCA’s response. If you are interested in certifiedDCA’s response to me let me know and I will post it.
Here is pharma-DCA’s response to me.
Hello Michael
Thanks for the response; Pharma-dca.com is part of the AWP group of internet companies.
We do however agree that the vast amount of Sodium Dichloroacetate for sale originates in China.
We have been concerned regarding this issue but as you will appreciate have no control over the purchasing by individuals who unfortunately have not the knowledge or realization of product source.
AWP for many years has had its own in-house fully equipped laboratory and routinely sample every batch of product produced.
All our Sodium Dichloroacetate is produced within the UK to exacting standards; a typical analysis would be as follows:
All product is batch produced and the batch number displayed on the product label for maximum quality control.
An inductively Coupled Plasma Mass Spectrometer offers the initial indication of the product quality, we have available if required a Perkins FTIR Spectrometer, a Hewlett Packard Gas Chromatograph plus other equipment. Finally a sample of the finished product receives a quantitive analysis by titration.
Only product that meets our strict guidelines is sent for packaging etc.
Finally if you look at our website you will observe that we also produce potassium dichloroacetate, we have not seen this anywhere else including China.
We welcome anyone to have our product analyzed on their own behalf
Some feel placing DCA in a freezer is important, most seem to feel just refrigeration is fine. It is claimed the freezer keeps DCA fresher for much longer, but from a practical point of view, you will go through a 100 g bottle rapidly enough that it does not matter. We keep it in the refrigerator. We do not worry about with or between meals. Benfotiamine is taken in the morning around the time DCA is taken. Might be taken at the same time or at a different time, same with thiamine at night.
Friday, 14 July 2017
My father's GBM
My father was diagnosed with GBM on 4/15 and he had a total resection surgery on 4/17. I've been researching pretty much non-stop every since. I watched the surviving terminal cancer movie, read Ben Williams book, have been scouring the internet gathering as much information as possible and this is how I ended up here.
Here's all the information I have on my fathers tumor and the treatment and supplements he is on to date:
Genetic testing: MGMT was not detected (negative) unmethylated
IDH1 and IDH2 were not detected (negative) as well
It is EGFR amplified - which qualified him for ABT-414 clinical trial.
He is currently in the trial and has some symptoms which lead us to believe he is getting the actual drug and not the placebo.
He finished up the standard treatment of Radiation and Chemotherapy a few weeks ago.
He is taking Keppra and a PPI daily
List of supplements: Cannabis oil, 20 mg melatonin, 800 mg curcubrain, reishi and coriolus mushroom supplement, 500 mg Boswellia extract, 400 mg green tea extract, 200 mg resveratrol, 200 mcg selenium, 10000 IU vitamin D3, Hemp seed and flax seed oil.
Also drinking fruit and veggie smoothies daily.
These are the off label drugs that I recently received and plan on having him start in a couple days.
These are the off label drugs that I recently received and plan on having him start in a couple days.
Disulfiram-125 mg a day for the first week, then 250 mg daily
Chloroquine- 250 mg daily
Celebrex- 200 mg twice daily
Metformin- 500 mg once daily, titrating up to twice daily, then 3 times daily
Doxycycline 100 mg twice daily
Propranolol 60-80mg daily
Lipitor
DCA 5mg/kg per day, titrating up to 12-15mg/kg.
LDN (low dose naltrexone) start with 2mg nightly titrating up to 4.5mg
I have a few questions:
1.How does the dosing and schedule of the off label drugs look? Anything I should add or subtract?
2. I know Disulfiram and DCA can cause neuropathy, should they not be taken together?
3. Should the green tea extract pills be avoided while on DCA?
4. The doxycycline I have is Dox T-SL (Doxycycline 100 mg / Lactic Acid 5 billion spores)
It says "DOXT-SL contains Doxycycline along with 5 billion spores of lactobacillus sporogenes."
Would the lactic acid cause a problem?
5. Most of the research I've done says statins are beneficial, but I've also an article saying they should be avoided. Should they be used or avoided?
If he does take the Celebrex, any recommendations on dose?
6. The Naltrexone pills I have are 50 mg. I've seen people dissolve them in 50mg of water and then use a syringe to suck up desired amount in mg. Is this advisable? Some people say this will cause inconsistent doses, but I don't know another way.
7. I've read that since his GBM is unmethylated and EGFR amplified that a metronomic chemo scheduling would be more beneficial than standard chemo treatment. We meet with my fathers oncologist next week to take a scan and discuss the future game plan. Does anyone have any recommendations on how to try and convince his dr. to prescribe the metronomic dosing schedule.
Any help or suggestions would be greatly appreciated. Like I said, I've been doing a ton of research and sometimes it seems like the more I do, the more confused I get.
Saturday, 8 July 2017
help with Dex effects
my husband had a second recurrence at the end of May. Further surgery is not an option (he had awake craniotomy with Gliolan in February for first recurrence, so we were very disappointed that it came back so quickly). He has been on 16mg per day of dexamethasone since May 30. We are trying to make the most of every day but the fatigue is extreme and he has weakness and visible muscle wastage in his arms and legs. Does anyone have any tips please on how to counteract the fatigue? He is 47, first diagnosed August 2015.
Any help much appreciated.
Any help much appreciated.
Friday, 7 July 2017
Updated statistics from Duke's modified poliovirus trial for recurrent GBM
- As of 2/01/2017, 52 pts were treated on study (1 each at DL1 and DL3, 7 at DL2, 2 at DL4, 4 at DL5, 24 at DL-1 and 13 at DL-2)
- 20.8% of pts remain alive at 36-month post PVSRIPO infusion, compared to 4% of an historical control.
- Four pts remain alive more than 22 months post treatment without having received any additional intervention following PVSRIPO at 57.5+, 56.4+, 27.9+ and 23.2+ months.
An important thing to keep in mind is that the patients in this phase 1 trial were treated with various doses of the virus. We can expect future trials that move forward with the approximately optimal dose to have better overall results than this trial. The first patient in this trial is now 5 years in remission.
Sativex (THC + CBD) plus temozolomide for recurrent GBM
This was mentioned in the comments a while back (February), but I feel these findings are significant enough to have their own post.
The original press release by GW pharmaceuticals came out on February 7.
The data was also published for the 2017 ASCO conference (click here).
"Median survival in the placebo group was 369 days, and > 550 days in the CBD:THC treatment group (NS) and 1 year survival was 83% and 56% in the CBD:THC and placebo groups, respectively (p = 0.042). "
The original press release by GW pharmaceuticals came out on February 7.
The data was also published for the 2017 ASCO conference (click here).
"Median survival in the placebo group was 369 days, and > 550 days in the CBD:THC treatment group (NS) and 1 year survival was 83% and 56% in the CBD:THC and placebo groups, respectively (p = 0.042). "
Even with the small numbers of patients (12 patients in the Sativex + TMZ group, 9 patients in the placebo + TMZ group), the difference in survival at one year still managed to achieve statistical significance.
Sativex (nabiximols) is available in Canada and Europe.
Complete responses to Toca 511 for IDH1 mutant gliomas
This was an abstract from this year's ASCO conference.
Durable complete responses observed in IDH1 mutated high grade glioma at first recurrence undergoing treatment with Toca 511 and Toca FC (click here for the abstract)
"All 4 IDH1 mt patients treated at 1st recurrence had CRs [complete responses]" !
Durable complete responses observed in IDH1 mutated high grade glioma at first recurrence undergoing treatment with Toca 511 and Toca FC (click here for the abstract)
Thursday, 6 July 2017
Is SWI part of standard MRI imaging?
I recently read that SWI can reliably determine regrowth from pseudo-recurrence. If this is the case why are there so many concerns about pseudo-recurrence? Is SWI not used standardly? Does it have pitfalls? Does it require use of contrast agent? (I haven't had MRI with contrast yet, due to pregnancy, so I'm wondering about "establishing a baseline" from which to measure my tumour going forward.)
Monday, 3 July 2017
IDH1-inhibitor drugs?
Hello all,
I've not fully understood how mIDH1-inhibitors work? I know they reduce 2-HG levels but does that lead to tumour regression, or is there some other mechanism simultaneously?
I've been looking into different mIDH1-inhibitor trials, but have doubts if they work as monotherapy?
Br,
Juha
I've not fully understood how mIDH1-inhibitors work? I know they reduce 2-HG levels but does that lead to tumour regression, or is there some other mechanism simultaneously?
I've been looking into different mIDH1-inhibitor trials, but have doubts if they work as monotherapy?
Br,
Juha
Getting Second Opinion - Planning for recurrence
Hi all,
My Dad was diagnosed in Nov. 2016 with GBM (MGMT methylated, Positive for 1p Deletion, NOT IDH1/2).
He has completed standard chemo-radiation and is about to start his 6th cycle of monthly TMZ. We have had (2) Avastin infusions so far (hoping to keep this as minimal as possible) to help us wean off decadron, now down to 1mg per day.
As of our last MRI my Dad is considered "Progression Free - Post Avastin".
We are seeing Dr. Butowski at UCSF. He is very intelligent and has been willing to discuss our cocktail decisions. He simply states what is safe, his belief of what works and what does not based on research, and then let's us make our decision.
We do not want to switch NO's, but so far in this journey he has not been interested in any clinical trials (for my Dad) happening anywhere on the West Coast. He feels we stick with TMZ and sporadic Avastin infusions until (statistically likely) a recurrence appears. At that point we make a plan based on what is found...
I don't feel comfortable with this plan, I want to stay ahead of this. I want to start reaching out to various clinical trials of any phase and see what makes the most sense. Dr. Butowski leads much of the research at UCSF and has seen many trials do nothing and/or have very negative side effects on patients so he is more cautious than other NOs. I know this is something to be thankful for, but also very frustrating.
I would like to setup a consultation with another NO from a leading brain tumor center anywhere in the world to sit with and run through our situation for as long as I can get. I would love if members from around the world could list NO's they admire and respect.
Might actually be worth developing a shared Google Sheets for Stephen W Library listing all NO's with forum members ratings/opinions.
Any advice is appreciated.
Thank you and never give up
Ari
Oakland, California
My Dad was diagnosed in Nov. 2016 with GBM (MGMT methylated, Positive for 1p Deletion, NOT IDH1/2).
He has completed standard chemo-radiation and is about to start his 6th cycle of monthly TMZ. We have had (2) Avastin infusions so far (hoping to keep this as minimal as possible) to help us wean off decadron, now down to 1mg per day.
As of our last MRI my Dad is considered "Progression Free - Post Avastin".
We are seeing Dr. Butowski at UCSF. He is very intelligent and has been willing to discuss our cocktail decisions. He simply states what is safe, his belief of what works and what does not based on research, and then let's us make our decision.
We do not want to switch NO's, but so far in this journey he has not been interested in any clinical trials (for my Dad) happening anywhere on the West Coast. He feels we stick with TMZ and sporadic Avastin infusions until (statistically likely) a recurrence appears. At that point we make a plan based on what is found...
I don't feel comfortable with this plan, I want to stay ahead of this. I want to start reaching out to various clinical trials of any phase and see what makes the most sense. Dr. Butowski leads much of the research at UCSF and has seen many trials do nothing and/or have very negative side effects on patients so he is more cautious than other NOs. I know this is something to be thankful for, but also very frustrating.
I would like to setup a consultation with another NO from a leading brain tumor center anywhere in the world to sit with and run through our situation for as long as I can get. I would love if members from around the world could list NO's they admire and respect.
Might actually be worth developing a shared Google Sheets for Stephen W Library listing all NO's with forum members ratings/opinions.
Any advice is appreciated.
Thank you and never give up
Ari
Oakland, California
Sunday, 2 July 2017
Avastin Fatigue sideffects
Hello, my husband's last MRI following his 2nd round of adjuvant TMZ showed his right temporal lobe gbm increased in size by 50% as well as a new tumor on left side on anterior horn of left lateral ventricle. Our NO recommended Avastin
only at 1/2 dose, so we had first infusion on June 5th then another on June 19th. My husband has declined significantly mentally and physically since then. He is sleeping 20-22 hrs a day, and today his legs seemed to give out on him and it took my son and I several hours to get him back into bed bc of confusion he wouldn't trust us or let us help him. It was heartbreaking. Our NO is saying it will take 2 more treatments to see if it is working....does this sound right? He is suppose to get 3rd infusion tomorrow, but I don't even know if I will physically be able to get him there, so that may be answer in itself. I just want to know I did all I could. Do you all think if he was going to respond he would've done so by now or shown some improvement? Thank you for your help.
only at 1/2 dose, so we had first infusion on June 5th then another on June 19th. My husband has declined significantly mentally and physically since then. He is sleeping 20-22 hrs a day, and today his legs seemed to give out on him and it took my son and I several hours to get him back into bed bc of confusion he wouldn't trust us or let us help him. It was heartbreaking. Our NO is saying it will take 2 more treatments to see if it is working....does this sound right? He is suppose to get 3rd infusion tomorrow, but I don't even know if I will physically be able to get him there, so that may be answer in itself. I just want to know I did all I could. Do you all think if he was going to respond he would've done so by now or shown some improvement? Thank you for your help.
Saturday, 1 July 2017
Boswellia Serrata During Standard of Care
Any thoughts about using 4200 mg of Boswellia Serrata during SOC? Received conflicting messages from oncology pharmacists regarding interference with TMZ. Any information or experience would be appreciated.
Thank you.
Thank you.
Randomized trial comparing 6 to 12 cycles of TMZ
Many studies have compared 6 cycles of monthly temzolomide to extended temozolomide for newly diagnosed GBM. However, all of those studies have been retrospective in nature (they were not designed as prospective clinical trials randomizing patients to either 6 or 12 months of monthly TMZ).
A small (20 patients in each arm), but randomized trial was published recently by an Indian group. The result was a 4 month increase in median progression-free survival in the 12 month arm, and a >8 month increase in median overall survival (15.4 months versus 23.8 months), measured from diagnosis.
Patients in this trial were between the ages of 18 and 65, with KPS equal to or over 70. Unfortunately, there was no information (and consequently no stratification by) MGMT status, which limits the significance of the study, as the authors readily admit. "One limitation of our study is the small sample size of patients and lack of information on MGMT methylation status of patients." However, this is the first randomized trial for newly diagnosed GBM comparing 6 cycles to 12 cycles of monthly temozolomide treatment.
Download PDF by clicking here
A small (20 patients in each arm), but randomized trial was published recently by an Indian group. The result was a 4 month increase in median progression-free survival in the 12 month arm, and a >8 month increase in median overall survival (15.4 months versus 23.8 months), measured from diagnosis.
Patients in this trial were between the ages of 18 and 65, with KPS equal to or over 70. Unfortunately, there was no information (and consequently no stratification by) MGMT status, which limits the significance of the study, as the authors readily admit. "One limitation of our study is the small sample size of patients and lack of information on MGMT methylation status of patients." However, this is the first randomized trial for newly diagnosed GBM comparing 6 cycles to 12 cycles of monthly temozolomide treatment.
Download PDF by clicking here
Subscribe to:
Posts (Atom)